
IOL Services - Defocus Curves
Background
Presbyopia-correcting intraocular lenses (IOLs) are designed to reduce dependence on reading spectacles by providing useful vision over a range of distances. The 'defocus curve' assessment technique uses a series of positive and negative powered lenses to simulate different distances over which the subject's visual acuity (VA) is evaluated (Figure 1).
Uses
This technique has been used to compare visual performance in patients implanted with monofocal and accommodating IOLs,1 and between different multifocal IOL platforms.2-4
Conventional tests
Defocus curves are often plotted in a sequential lens order using the same target letters which leads to inaccuracies. Similarly, measurements are typically made under a single set of lighting conditions and using just high-contrast letters. Due to a lack of standardised techniques, a wide range of values can be reported for a given IOL platform.
Our approach
An 'ideal' test should evaluate VA with letters of differing contrast levels under both photopic and mesopic conditions to fully appreciate visual performance for different viewing conditions. Furthermore, the test lenses and target letters should be randomised to reduce potential learning effects.5 A correction for a change in image size through the additional test lenses is also required when analysing the results.6 Defocus curve metrics, such as the area under the curve,4,7 are useful for comparing different presbyopia-correcting technologies. The optimal range of lens powers required to rapidly define the amplitude of accommodation of all presbyopia-correcting IOLs is currently unclear.
We are developing rapid defocus techniques to reduce the burden on both patients and clinicians and to allow time for measurements at different contrasts, different luminance levels and/or monocularly/binocularly.
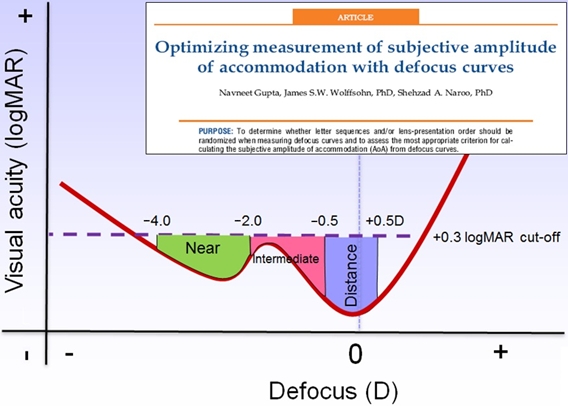
Figure 1. A typical example of a defocus curve for a multifocal IOL.
References
- Cleary G, Spalton DJ & Marshall J. Pilot study of new focus-shift accommodating intraocular lens. J Cataract Refract Surg. 2010; 36:762-770.
- Cillino S, Casuccio A, Di Pace F, et al. One-year outcomes with new-generation multifocal intraocular lenses. Ophthalmology. 2008; 115:1508-1516.
- Toto L, Falconio G, Vecchiarino L, et al. Visual performance and biocompatibility of 2 multifocal diffractive IOLs: six-month comparative study. J Cataract Refract Surg. 2007; 33:1419-1425.
- Wolffsohn JS, Buckhurst PJ, Shah S, Naroo SA & Davies LN. Evaluation of Multifocal Intraocular Lens Defocus Curves. Invest Ophthalmol Vis Sci. 2011; 52:(E-Abstract 4772).
- Gupta N, Naroo SA & Wolffsohn JS. Is randomisation necessary for measuring defocus curves in pre-presbyopes? Cont Lens Anterior Eye. 2007; 30:119-124.
- Steinert RF, Post CT, Jr., Brint SF, et al. A prospective, randomized, double-masked comparison of a zonal-progressive multifocal intraocular lens and a monofocal intraocular lens. Ophthalmology. 1992;99:853-860; discussion 860-861.
- Trager MJ, Vagefi RM & McLeod SD. A Mathematical Model for Estimating Degree of Accommodation by Defocus Curves. Invest Ophthalmol Vis Sci. 2005; 46:B691 (E-Abstract 717).